

Lithium, the Essential Trace Element
The key element against brain fog, long-COVID/post-vac syndrome, chronic fatigue syndrome, depression, Alzheimer's – and even indoctrination?

The ability to live a long and healthy life depends on the optimal functioning of both our mental and physical immune systems. These systems do not operate independently; they share common needs (species-specific lifestyle, micronutrients, etc.) and mutually influence each other. The mental immune system includes our experiential knowledge, our natural curiosity, and our social and planning skills - fundamental functions of our autobiographical memory center (hippocampus). The lifelong production of new brain cells in the hippocampus (adult hippocampal neurogenesis) is essential for maintaining its function and thus mental immunity. Conversely, the function of the body's immune system depends on a balanced immune response to pathogens or injury. This involves both the initial activation of pro-inflammatory messengers, where necessary, and the equally effective deactivation and activation of anti-inflammatory messengers at the appropriate time. These, in turn, serve to repair damaged cells and restore regulated balance (homeostasis).
The acute release of pro-inflammatory messengers inhibits neurogenesis in the adult hippocampus, a process that may be beneficial to the healing process, but becomes problematic when this neuroinflammatory release of these cytokines becomes chronic and continuously damages the mental immune system. This is the beginning of a vicious cycle that is difficult to break: The long-term dysfunction of the hippocampus leads to reduced psychological resilience, which triggers an excessive and chronic stress response, which in turn overactivates the brain's immune system and leads to an increased and particularly persistent release of pro-inflammatory messengers.

Microdosing lithium can reduce the risk of entering this life-threatening cycle in the first place. A slightly higher dosage even offers the legitimate hope of breaking an existing cycle. The catch: Although there is ample scientific evidence that lithium, in addition to its well-known therapeutic benefits, is also an essential trace element, it is not yet recognized as such and, for example, cannot be marketed as a dietary supplement in most EU member states. Although microdosed lithium is available in the U.S. as OCT, its non-essential status (and the misperceived risk of side effects known from macrodosing in the treatment from bipolar disorder) inhibits its wider use as a natural preventative measure against chronic inflammation.
Lithium, Essential for Both the Mental and Physical Immune Systems
There are numerous arguments in favour of lithium being an essential trace element, even though it is not yet recognized as such. A deficiency can lead to faulty functioning not only of the mental but also of the physical immune system. In my book "Alzheimer's is Curable," published in 2015 (so far only in German), I pointed out the intolerable situation for our health maintenance that lithium is not officially recognized as an essential trace element. The significance of microdosed lithium for mental health was also detailed in my scientific article Unified Theory of Alzheimer's Disease (UTAD): Implications for Prevention and Curative Therapy, published in July 2016.i Lithium serves a variety of functions in the body, as I will show in a few examples here. Not only does it help reduce the risk of Alzheimer's dementia or depression. Even a very small increase in lithium intake (due to slightly different concentrations in tap water) can prolong life expectancy and may even be lifesaving by reducing the suicide rate, as we have known for several years from Japanese and many other studies.ii With around 730,000 officially confirmed suicides worldwide in 2019 alone (the number of unreported cases is always higher), a simple preventive measure, such as microdosed lithium would actually be longed for, if we didn't already know from studies that we could rely on this powerful ally in the fight against this serious global problem; especially since 2020, when the suicide rate has risen drastically once again (most likely due to the coronavirus measures and the constant fear propaganda).iii My understanding of the connection between lithium deficiency, persistent fear propaganda and increased rates of despair and suicide is that without a functioning mental immune system we are hardly able to correctly assess the constantly exaggerated threat scenarios (a core competence of the hippocampus, as I explain in detail in my book The Indoctrinated Brain). The bitter realization of recent years that our health care system is rather a disease system can also, with a healthy hippocampus, be understood as a fruitful insight that does not leave us stunned, but rather encourages us to focus more on personal responsibility and to work toward natural health that does not make us dependent on the pharmaceutical cartels. However, if this does not succeed and stress gets out of hand, the self-destructive vicious cycle of neuroinflammation mentioned earlier (and illustrated and explained in detail in the diagram below) occurs, which could be interrupted by low-dose lithium.
However, lithium should be considered a vital trace element not only because of its significant effect on mental health, as I explained in my book The Corona Syndrome in 2021. Lithium should also have earned this status because of its multipotency in regulating the body's immune system. This was known long before the SARS-CoV-2 pandemic.iv It was already known that lithium reduces the infectivity of a variety of DNA and RNA viruses. And particularly relevant for SARS-CoV-2: It was shown in 2007 that lithium specifically inhibits the growth of coronaviruses.v In addition to its various antiviral properties, this trace element modulates or reduces the activity of several important molecular signal transducers, such as GSK3 in particular. This is also the reason why not only vitamin D deficiency but also lithium deficiency enables the development of the so-called cytokine storm (an overreaction of the immune system), which is the actual reason for the severe to fatal course of SARS-CoV-2: It has been known since the beginning of the pandemic that it is not the virus itself that kills, but a misdirected and therefore overreacting immune system - but politicians and the media generally fail to mention how easy it is for everyone to constitutionally protect themselves against such overreactions. As early as June 2021 in my book The Corona Syndrome (in German language only), I suggested lithium as the means of choice to prevent the life-threatening effects of a SARS-CoV-2 infection, in addition to adequate vitamin D supplementation for the population. There were several groups of scientists and doctors who were pointing this out as well in their scientific publications. vi
But these suggestions were generally ignored, despite the fact that a first successful clinical application of lithium in six separate COVID-19 cases was published in August 2020. Although the causal relationship indicated in the publication should have been regarded as a sensation, this inexpensive, readily available (and non-patentable) trace element did not receive the life-saving attention it deserved.vii The authors of this study justified their approach and explained the positive results as follows: "Lithium has shown the capacity to: a) inhibit the replication of several types of viruses, some of which are similar to the SARS-CoV-2 virus, b) increase the immune response by reducing lymphopenia [lack of immune cells due to their overconsumption in severe COVID-19 courses], and c) reduce inflammation by preventing or reducing the cytokine storm [the primary cause of severe courses, as mentioned above]." However, the success of the study and the clarity of the science behind it paved the way for a larger, placebo-controlled clinical trial to be published in 2022.viii The results were remarkable: compared to the COVID-19 patients in the control group who did not receive lithium, the length of hospital stay in the lithium group was halved (!). The disease stabilized and the patients improved so quickly on lithium that none had to be admitted to intensive care. In the control group, two out of 15 patients required intensive care and one eventually died.
Lithium is Effective Even in Microdoses
Lithium is an essential trace element as it fulfills the crucial criterion of regulating, even in micro quantities, cellular processes that are crucial for healthy physical and mental development and for maintaining our health.ix To understand the highly efficient effect of lithium, it is necessary to imagine every single cell in our body as an information-processing microprocessor that receives signals from its environment through receptors on the cell surface (and some inside the cell), evaluates them, and finally sends its "findings" back to the rest of the organism in the form of new signals. This highly complex control program is vital not only for individual cells, but also for the organs they form and, ultimately, for our very existence.
The activity of master regulators like GSK3, which receive and process signals within the cell are often regulated by trace elements such as lithium (but also magnesium, for example). The concentration of these trace elements is therefore crucial not only for our well-being, but also for our survival. There is strong evidence that GSK3 has been controlling essential biological processes for an astonishing 500 million years or more.x Even the first single-celled microorganisms must have possessed the GSK3 protein. And this is so amazing because there is strong evidence that the supposedly non-essential lithium was already contributing in micro quantities to the activity and function of GSK3 and to cellular and organic balance (homeostasis) so early in evolution. As one of the oldest signaling regulators in evolutionary history, GSK3 not only plays a central role in the "cellular processor" of countless life forms, but also influences the function of more than 80 proteins (many of which are signal transducers themselves).
Microdosed Lithium: The Key Element Against Post-Spike Syndrome (Long-COVID and Post-Vac), Chronic Fatigue, Depression and Alzheimer's?
As a master regulator, GSK3 is responsible for controlling the physical as well as the mental immune system. When GSK3 is activated, pro-inflammatory mediators are released; when the master regulator is inactive, anti-inflammatory mediators are produced and released. Lithium reduces the activity or inhibits the activation of GSK3 and thus has an anti-inflammatory effect. Numerous studies have shown that even very low blood levels of lithium reduce the risk of developing chronic neuroinflammation. Therefore, in my opinion, low-dose lithium can and should be used to try to break the vicious circle of neuroinflammation described below, which is set in motion by chronic anxiety scenarios, but also by the S1 subunit of the spike protein (both after SARS-CoV-2 infection and after spike mRNA injection). According to scientifically convincing studies, this vicious circle, as shown in the following diagram, is responsible for the "brain fog" phenomenon and thus for the psychological effects of long-COVID and post-VAC syndrome, which I summarize under the term Spikeopathy (or post-spike syndrome) because of the common trigger.
In the following, we will go through the steps in the diagram below. I have deliberately refrained from using the names or abbreviations of some of the signaling molecules if they do not add to the understanding. At the beginning of each numbered paragraph, I will summarize each step in a generally understandable but abbreviated way. If you find the more detailed information below too technical, you can skip to the next section. Keep reading for a clear and straightforward explanation of lithium's importance, located further below.
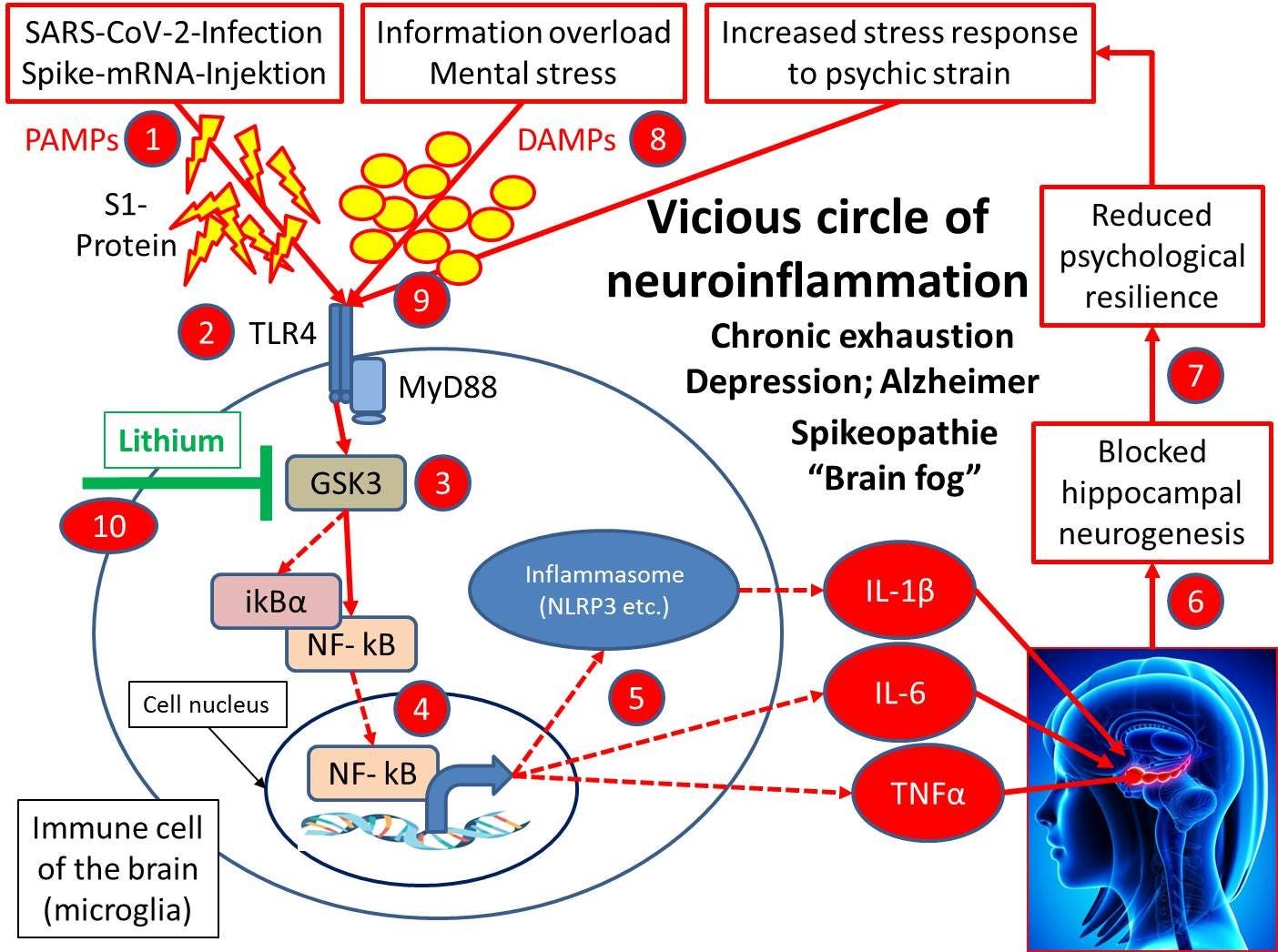
Both infection with SARS-CoV-2 and injection of genetic material (mRNA) encoding the spike protein of SARS-CoV-2 lead to accumulation of the S1 subunit of the spike protein in the brain. The nearly identical neuropathologic consequences (Long-COVID or Post-Vac) are now referred to as Spikeopathy.xi
Expansion: An autopsy study shows this clearly.xii The authors write, among other things: „The [experimental] pike protein alone caused cell death in the brain,highlighting a direct effect on brain tissue Furthermore, we observed the presence of spike protein in the skull of deceased long after their COVID-19 infection, suggesting that the spike’s persistence may contribute to long-term neurological symptoms.”
A first step towards the neuropathological effects and psychological manifestations of Spikeopathy begins with the binding of the S1 subunit or protein to a sensor molecule (TLR4), which belongs to the evolutionarily ancient family of so-called "danger recognition receptors". The pathogen sensor molecule is known as TLR4 (toll-like receptor). It is located on the cell surface of microglia, the immune cells of the brain.xiii By activating TLR4, the danger posed by the pathogen is recognized and reported to the entire immune system via pro-inflammatory messengers. We will take a closer look at the signaling chain below.
Expansion: Receptors such as TLR4 are part of the innate immune system, which has been optimized over hundreds of millions of years of evolution in complex organisms to recognize basic patterns in pathogens (viruses, bacteria or fungi) and activate the adaptive immune system by releasing pro-inflammatory cytokines. Of the many different TLRs that humans possess, almost all family members recognize certain parts of coronaviruses, including SARS-CoV-2.xiv These recognized common patterns are referred to as PAMPs (Pathogen-Associated Molecular Patterns). Since all coronaviruses have spikes, they are also commonly recognized. The fact that both mice and humans recognize spike proteins of coronaviruses as PAMPs via TLR4 (and many other TLRs) indicates that this class of viruses has existed as pathogens for many millions of years and that an innate defense strategy (like TLR recognition) has already evolved in the common ancestor of mice and humans.
The transmitted signal is forwarded to and activates the master regulator GSK3.
Expansion: Recognition of the S1 subunit by TLR4 leads to activation of a signaling cascade that is mediated by the multifunctional intracellular master regulator GSK3. GSK3 is also highly conserved in evolutionary terms and had essential functions in the common ancestor of humans and amoeba-like protozoa several hundred million years ago, which could still be influenced by lithium (!) in the same way in both organisms today - and thus very likely even back then - in a way that was crucial for life.xv
The resulting activation of GSK3 then triggers another signal that leads to the production and release of pro-inflammatory mediators by the cells.
Expansion: GSK3, activated by the S1 protein activated TLR4, in turn activates the immunological transcription factor NF-kB, in part by dissociating it from its inhibitor (iKBα). NF-kB then migrates to the nucleus, where it turns on a long list of genes that encode pro-inflammatory cytokines. These genes include those for IL-6, TNFα and NLRP3. The latter is an essential component of the inflammosome. The inflammosome is a multiprotein complex of the innate immune system that is also responsible for activating inflammatory responses, such as the release of the pro-inflammatory cytokine IL-1β.
The pro-inflammatory mediators (such as IL-1β, IL-6, and TNFα) now released in the brain tissue block the production of new neurons in the hippocampus, which is necessary to maintain many of its autobiographical memory functions.xvi In the case of acute inflammation, this inhibition is not a serious problem; it may even be an evolutionary advantage, since it (psychologically) immobilizes the patient until the acute infection is over, thus aiding the healing process. However, if the neuroinflammation becomes chronic, e.g. due to the permanent presence of a spike protein (or its S1 subunit) in the brain, or due to equally chronic psychological stress, the hippocampus suffers considerable damage.
Expansion: Inhibition of GSK3 activity in microglia is common to almost all types of antidepressants and is most likely their central mechanism of action. Ultimately, this inhibition leads directly and indirectly to an increase in hippocampal neurogenesis, which is the actual antidepressant effect.xvii
The chronic loss of function of the hippocampal memory center due to permanently impaired hippocampal neurogenesis explains a large part of the post-spike symptoms. These include depressive moods, drive problems, memory disorders and increased anxiety symptoms as a result of reduced psychological resilience. The frequently described inability to concentrate (brain fog) in connection with long-COVID or post-vac is also highly likely to have a causal relationship.
Expansion: This is consistent with the fact that people with mutations in the TLR4 gene that increase its activity are more likely to develop long-COVID symptoms than the rest of the population. In contrast, individuals with mutations that decrease the activity of their TLR4 gene have a lower risk of long-COVID. This relationship has been confirmed as causal in animal models, suggesting that Spikeopathy (brain fog, etc.) most likely results from the signaling cascade shown here.xviii
The neuroinflammatory inhibition of hippocampal neurogenesis and the resulting reduction in mental resilience initially increases the risk of developing depression and, in the long term, even Alzheimer's disease or hippocampal dementia, which are its main causes.xix
Expansion: Due to the mechanisms shown here, the S1 subunit is also a trigger for the enormous increase in new cases of these two neurological diseases since 2020 (in addition to many other factors, which I describe in detail in my book The Indoctrinated Brain). The molecular connections, as shown in the diagram above, are now well understood.xx
However, the neuroinflammatory vicious circle can be triggered not only by pathogens or their products, but also by constant overstimulation or chronic (neurotoxic) stress.
As a result of neurotoxic cell damage, molecules are released from inside the cell. Some of these are referred to as DAMPs in analogy to the PAMPs mentioned above: Danger-Associated Molecular Patterns.xxi They also activate TLR4 and can set the vicious circle of neuroinflammation in motion. The consequences are depression and, in the long term, even Alzheimer's disease. However, if the neuroinflammatory vicious circle (through DAMPs or PAMPs) has already been set in motion, a challenge or even moderate mental stress, which under other circumstances can have a positive stimulating effect, can lead to excessive DAMP release in a state of reduced mental resilience.
Expansion: In fact, psychological trauma (threats, isolation, fear-inducing events, loss of a partner) is more likely to result in pre- or post-traumatic stress disorder (including hippocampal shrinkage), the higher the measurable levels of these pro-inflammatory messengers. This suggests a causal relationship between these disorders and neuroinflammatory processes. This causal relationship can be clearly seen in the graph.
Like the spike and S1 proteins (which belong to the PAMP group), DAMPs are also potent activators of the above-mentioned danger recognition sensor in the brain (TLR4). Both can therefore be at the beginning of this vicious circle and thus ensure via the same signaling pathway that inflammation-promoting messenger substances are constantly and increasingly released. DAMPs and PAMPs, i.e. psychological stress (fear propaganda) as well as exposure to products of pathogens (S1 protein through infection or mRNA injection program) can maintain the vicious circle of neuroinflammation and even reinforce each other.
Expansion: The activation of the hazard recognition signaling chain (via TLR4) by both mechanisms (spikes/PAMPs and neurotoxic stress products/DAMPs) shown in the graphic also provides an explanation for why people who were already under severe psychological stress (due to depression, anxiety, worry, perceived stress and loneliness) before SARS-CoV-2 infection or spike mRNA injections have been shown to be more likely to develop post-spike syndrome.xxii The reason: Both influences intensify the neuroinflammatory disease process, as has been shown in animal experiments. This is known as priming. So if you combine spike exposure (PAMPs) with psychological stress (DAMPs), as has been increasingly the case since 2020, and then take into account the spike mRNA injection program from 2021, which has further exacerbated the problem described, the risk of developing Spikeopathy, as described in The Indoctrinated Brain, is once again significantly increased.
Because the neuroinflammatory cycle is self-perpetuating, can be exacerbated, and is devastating to mental health, it is extremely important to break it as quickly and effectively as possible. Because the trace element lithium down-regulates the activity of the master regulator GSK3, it helps interrupt this neuroinflammatory signaling chain.As a result, the production of neuroinflammatory mediators is reduced. As the activity of the master regulator (GSK3) is reduced, anti-inflammatory messengers are actually activated. AAs a result, hippocampal neurogenesis is no longer blocked, but actually activated by lithium (more on this below). Side effects are not expected, as lithium in trace concentrations acts as a natural regulator (as opposed to an almost complete blockade of GSK3 function, as is achieved with macro doses in bipolar disorder).xxiii You can read more about what lithium levels are considered "natural" later.
With this in mind, the State University of New York at Buffalo in the USA began a randomized, placebo-controlled study with low-dose lithium in patients with post-spike symptoms (such as brain fog) in November 2022.xxiv Thomas J. Guttuso, physician and professor of neurology at the Jacobs School of Medicine and Biomedical Sciences, is the leader of the study. The university's website and a press release explain what prompted the study: "Because long COVID [and thus Post-Spike] is believed to stem from chronic inflammation and lithium has known anti-inflammatory actions, Guttuso decided to recommend that a patient try low-dose lithium for persistent long COVID symptoms.”xxv The result was astonishing. „I was shocked when the patient saw improvement within a matter of days,”, Guttuso says in the university's press release. It also reports that during the pandemic, Spanish researchers were able to show that patients who were already taking lithium for bipolar disorder and were acutely infected with COVID-19 and hospitalized had better outcomes than patients who were not taking lithium. Guttuso's success led other doctors to start referring their long-COVID patients to him, according to the report: “Eventually, he was treating 10 additional long COVID patients with low-dose lithium; nine saw improvement from lithium. None [as expected] experienced side effects.“
Other Vital Effects of Lithium
When supplied in microdosed (essential) quantities, lithium regulates several other signaling molecules in addition to GSK3. This explains its diverse, health-promoting functions, which I would like to explain below.
Autophagy: Lithium activates both "microautophagy" and "autophagy", thereby stimulating a process of cell and tissue rejuvenation.xxvi This process breaks down misfolded proteins and obsolete cell organelles such as mitochondria (the powerhouses of our cells) that are no longer functioning optimally (e.g., when damaged by the spike protein). There is already compelling evidence that this cleaning process of autophagy also serves to eliminate viral components or reduce the severity of infection (SARS-CoV-2 is so successful in part because it disrupts or blocks this protective process of autophagy).xxvii In particular, active microautophagy might even support the degradation of the neurotoxic spike protein or its S1 subunit, thus helping to complete the healing process.xxviii Autophagy of spike-damaged mitochondria (in interaction with mitochondriogenesis, see next point) in turn supports the restoration of neuronal performance through improved energy metabolism. Finally, it prevents cell death (apoptosis) of damaged neurons.
Intermittent fasting or ketogenesis (also supported by coconut oil or ketogenic medium-chain fatty acids) also help to activate autophagy, as I have described in my books Alzheimer's is curable and The formula against Alzheimer's (unfortunately not yet published in English).
Mitochondriogenesis: Lithium activates (among other things by inhibiting GSK3) the so-called process of mitochondriogenesis, i.e. the production of new, healthy cellular power plants.xxix Because of the many other functions of mitochondria, the importance of this mechanism to our health and performance should not be underestimated.xxx This life-prolonging effect of lithium by improving mitochondrial function is probably true throughout the animal kingdom; at least it has been clearly demonstrated in a nematode, one of the simplest model organisms.xxxi Even there, lithium leads to a significant life extension.
Neurogenesis: As previously mentioned, lithium activates adult hippocampal neurogenesis by inhibiting GSK3 (and several other mechanisms)xxxii. Combined with the other effects of lithium mentioned above, this explains the antidepressant and Alzheimer's preventive properties of this underrated element.xxxiii In the early stages of Alzheimer's disease, a randomized clinical trial of microdosed lithium was able to stabilize the disease for 15 months, something no drug has been able to do.xxxiv
Systemic Prevention and Therapy of Neuroinflammation: All of the processes activated by lithium (inhibition of excessive inflammatory response and neuroinflammation, as well as activation of autophagy, mitochondriogenesis, and adult hippocampal neurogenesis) have an increased chance of success if they are supported by a healthy (species-appropriate) lifestyle, such as a healthy diet. Therefore, on my website I provide further information on how to support these health-promoting processes, for example with herbal agents. This is intended both as a beneficial measure against spike protein and to support hippocampal health in general (see my article on .
I plan an article on anti-spike herbs & herbs for hippocampal health. Subscribe to my Substack to be informed as soon as I put more information online for free:
Inadequate Lithium Intake in the General Population
Let's take a closer look at the numbers for a few paragraphs on the supply of lithium to the general population. In a study from 2020, an international team of researchers found a plasma concentration of 1 μg/L lithium (slightly rounded up) in a German study group with an average age of 61 years, in which no one was already taking lithium medication. However, the range of this value is only about 9 percent and depends on which foods are consumed more frequently (according to the authors, slightly higher values for potatoes and root vegetables).xxxv This value corresponds to the reference value of a Berlin laboratory, which is given as 0.35-1.45 μg/L.xxxvi It is therefore the defined "normal value" that can currently be achieved with a normal diet (in Germany, in this case).
The average dietary intake of lithium in Germany can be estimated using the results of a "mineral water study" conducted the previous year.xxxvii BA single dose of approximately 2.6, 260, or 2,600 μg lithium (found in various mineral waters) resulted in maximum lithium levels of approximately 1, 10, or 90 μg/L. However, these are maximum values measured 30 minutes after ingestion. The average lithium level over the entire day was only 0.3, 3, or 30 μg/L. This means that the amount of lithium ingested and the subsequent blood concentration correlate well. Therefore, if only one milligram (mg) of lithium is taken per day, the plasma level should be estimated to be about 10 μg/L, which is about 10 times the reference value of about 1 μg/L given above. This means that the daily dietary intake of lithium in the above study group was one tenth, or should be estimated at about 100 μg lithium.
However, the "normal value" mentioned above is neither natural nor species-appropriate. A diet rich in marine fish or seafood would be natural and normal in evolutionary terms, with a daily intake of several mg of lithium, i.e. at least ten times the usual amount today.xxxviii The "species-appropriate" lithium level would therefore be a factor of 10-20 above the currently measured "normality" or reference range, which therefore describes a lithium deficiency state that is common today. It is very likely that a daily intake of about 1 mg of lithium is sufficient to significantly reduce the risk of falling into a chronic neuroinflammatory process (see above), the neuropathological consequences of which include the development of depression, Alzheimer's dementia and some other mental illnesses (as well as an increased suicide rate). This amount of about 1 mg is therefore considered by many scientists to be an essential daily intake.xxxix
Since there is no reliable and recommended food source that accumulates enough lithium (sea fish and seafood are problematic due to toxin contamination and are not available in sufficient quantities for all people), and lithium is not approved as a dietary supplement in many countries, the only alternative to targeted supplementation is actually lithium-containing mineral water. However, this method of procurement is likely to be very expensive if you want to ensure stable lithium levels.xl This is due to the fact that free or unbound lithium ions, which are predominantly found in dissolved form in mineral water, have a high bioavailability (they are quickly and efficiently absorbed in the intestine), but are also very quickly excreted via the kidneys. Their half-life is only about 6 hours.xli This reduces the lithium level, which rises very quickly after ingestion, by a factor of about 16 per day with about four half-lives per day. In addition to the cost and the enormous amount of drinking water required depending on the lithium content, a high concentration in the water indicates a possible volcanic source. It cannot be ruled out that the water may also be contaminated with toxic metals such as uranium, as has been shown in some cases.xlii
So what is the alternative? I recommend getting lithium after consulting with a medical doctor and from pharmacies that guarantee high quality and purity. In some countries, the only way to get it without a prescription is illegally from abroad. However, I strongly advise against this, firstly because the quality of the product is not guaranteed, and secondly because a doctor's assessment is important for the therapeutic use of lithium, even in the "low dose" range (see below, for example, the treatment of "Spikeopathy (Long-COVID and Post-Vac)".
Lithium orotate, the better lithium?
Lithium orotate is superior to free lithium as found in mineral water, but also to other lithium salts. On the one hand, it ensures a more stable lithium level and, above all, higher concentrations in the brain.
Orotate is an endogenous molecule that is produced by the body only in small amounts and must be ingested daily with food to cover its needs. A deficiency results in impaired brain function, especially memory. In elderly rats, orotate supplementation has been shown to reverse orotate deficiency memory impairment.xliii It is used to produce genetic building blocks needed in the brain, particularly for the formation of new nerve cells in the hippocampus. This may explain the memory problems associated with deficiency. Orotate (and thus lithium orotate) is therefore efficiently transported across the blood-brain barrier by a special mechanism to counteract any impairment of brain function.
For the same reason, lithium bound to orotate is also well absorbed in the intestine (there is also a special transport mechanism for orotate). At the same time, however, lithium bound to orotate is excreted more slowly than free lithium ions. This leads to an estimated half-life of lithium orotate of more than one day, so that although the same amount of lithium (in the form of orotate) initially reaches a blood level comparable to that after ingestion of free lithium ions with mineral water, it remains elevated for much longer due to the binding to orotate.xliv To achieve the same average lithium level with mineral water, several liters would have to be drunk, depending on the lithium content, which not only drives up the cost, but is also unrealistic or impractical. Since this special transport mechanism across the blood-brain barrier is not available for free lithium or other lithium salts, lithium orotate is superior to these, especially if lithium is to contribute to improving brain function (for which, as described, orotate itself is also beneficial).xlv
Therefore, to achieve the same concentration in the brain and prevent neuroinflammation, it is sufficient to take smaller doses than with lithium salts such as lithium acetate or lithium carbonate, which have been used primarily for bipolar disorder. This also increases the threshold above which lithium intake would have toxic effects. According to animal studies, side effects are not observed even at concentrations many times higher than those required to prevent or break the neuroinflammatory vicious cycle: "In a 28-day, repeated-dose oral toxicity study, rats were administered 0, 100, 200, or 400 mg/kg body weight/day of lithium orotate by gavage. No toxicity or target organs were identified; therefore, a no observed adverse effect level was determined as 400 mg/kg body weight/day. These results are supportive of the lack of a postmarket safety signal from several decades of human consumption.“xlvi
Correct dosage of lithium orotate
Bipolar Disorder: To determine the optimal daily dose of lithium orotate, it is worth looking at the common practice of dosing other lithium salts, e.g., in the symptomatic treatment of bipolar disorder. Here, the target blood serum concentration is 0.8 to 1.2 mM (mmol/L), with more than 1.5 mM considered toxic. This results in a very low therapeutic range of about 1.5.xlvii The therapeutic range of a drug describes the relative distance between the therapeutic dose (or blood concentration) at which 50 percent of those treated experience a positive effect and a dose (blood concentration) that produces a toxic effect in 50 percent of those treated. Because the wider the therapeutic range of a drug, the safer it is, lithium treatment for bipolar disorder has many side effects and is not without danger. Even elevated serum lithium levels of 1.5-2.0 mM can have mild, though usually reversible, toxic effects on the kidneys, liver, heart, and endocrine glands. Serum levels above 2 mM may be associated with neurological symptoms, including cerebellar dysfunction. This narrow therapeutic window is one reason why most clinical laboratories specialize in determining lithium levels at this high concentration range and are unable to determine natural lithium levels, which are orders of magnitude lower. By way of comparison, let's consider the possibility of ingestion via drinking water: 1 mg of lithium ingested via mineral water results in a lithium level of approximately 10 μg/L or 0.0014 mM. This is only about one thousandth (!) of the toxic concentration of about 1.5 mM. To achieve blood levels of up to 1.0 mM, macrodosing of up to one gram of lithium carbonate or a lithium intake of about 200 mg per day may be necessary.
COVID-19: A slightly lower daily intake of a total of 80 mg of lithium (which would be about the molecular proportion of pure lithium in 400 mg of lithium carbonate) was enough to save the lives of all those seriously ill with COVID-19.xlviii It kept them out of intensive care and cut their hospital stays in half compared to the control group. However, the goal here was to prevent an acute cytokine storm triggered by a misguided immune system throughout the body or systemically, not just chronic neuroinflammation. This is probably the reason why a relatively high dosage was used or attempted here: After all, it was a matter of life and death, and the effect had to be fast and effective. I can well imagine that lower doses might have achieved the goal. Future studies will have to clarify this.
Spikeopathy (Long-COVID and Post-Vac): There is strong evidence that low-dose lithium should be able to break the vicious cycle of neuroinflammation caused by the S1 protein of SARS-CoV-2. A sufficient and low dose in this sense (low dose) means that about 5 mg of pure lithium might be sufficient. Please note that this information applies only to chemically pure lithium. If lithium is available in the form of lithium orotate, for example, the recommendation is to take about 115 mg of lithium orotate per day because this effectively means that you are taking 5 mg of pure lithium. This low dosage recommendation is also based on the better "brain accessibility" of lithium orotate compared to lithium acetate in the aforementioned COVID-19 study. For example, in an animal model of mania, 1/10 of the dose of lithium orotate was sufficient to achieve the same therapeutic effect as lithium carbonate (LiCO), which is also commonly used in medical practice. However, the lithium orotate formulation showed better efficacy and potency, because of select transport-mediated uptake and pentose pathway incorporation."xlix Because of this special transport mechanism, lithium orotate is not only recommended by me, but also discussed by other lithium specialists as a potential "superior option for lithium therapy" (of the future) when it comes to achieving the desired neurobiological effects.l
Although this therapeutic dosage of 5 mg of pure lithium (i.e., the effective proportion of lithium orotate) for Spikeopathy is 5 to 10 times higher than the preventive dosage (about 1 mg of pure lithium), it is still about 40 times lower than the dosage administered in conventional therapy for bipolar disorder (about 200 mg of pure lithium, see above). Side effects are therefore extremely unlikely, even at the therapeutic dose for Spikeopathy. However, even though the website of the Clinicum St. Georg states that "The use of lithium orotate in a dosage between 125-200 mg [with a corresponding lithium content of 5.5 to 8.6 mg] is simple and free of side effects", the attending physician should adjust the dosage if, for example, kidney disease is present (reduced or impaired excretion and thus prolonged half-life).li This is also the case during pregnancy and lactation or when prescription medications, especially antidepressants, are already being used. A therapeutic regimen of lithium for 1 to 3 months may also be sufficient to achieve the desired effect on neuroinflammation. After that, the amount taken can be reduced to what is essential (see next).
Essential requirement: Contrary to the literature and dietary guidelines, which continue to conceal the essential nature of lithium, a glance at the studies suffices to learn that an intake of approximately 1 mg of pure lithium is considered by scientists to be an essential requirement for the prevention of lithium-deficiency-related diseases (which ultimately include all so-called civilization diseases that develop on the basis of chronic inflammation). This also applies to the prevention of neuroinflammation in all chronic secondary diseases such as Spikeopathy, depression and Alzheimer's disease.
A microdose is about 23 mg of lithium orotate (which is 1 mg of pure lithium) or about 26 mg of lithium orotate mono-hydrate (the most common form of lithium orotate, which is also 1 mg of pure lithium) per day. However, even this small amount is currently only available by prescription in Germany and most EU member states, while it is legal in the US, as far as I know.
Sources of Lithium Orotate
In principle, any pharmacy can dispense lithium orotate in the form of an individually prepared prescription, which is always an individual mixture (that must be prescribed by a doctor in some countries). In Germany prescription drugs can only be manufactured and shipped after the original prescription has been received. Accordingly, a doctor would have to prescribe the capsules with 1 or 5 mg of lithium in the form of lithium orotate as needed, so that the pharmacy can prepare the corresponding prescription. The duration of use then determines the size of the prescription: 10 capsules, 30 capsules for one month, or 90 capsules for three months.
Disclaimer of Liability
All considerations presented here are based on publicly available documents and studies, most of which are also linked. Nevertheless, the author does not assume any liability for the contents and possible errors. This also applies to quantities. These are generally based on the requirements of an average adult. Deviations in dosage may result from lifestyle, gender, age, body size, pre-existing conditions, and especially from existing medications. Supplements should therefore only be taken after consultation with a trusted physician - the author assumes no liability for unauthorized use. It goes without saying that lithium preparations must be kept away from children, for example, due to their medicinal effects.
Literature references
i Nehls M: Unified theory of Alzheimer's disease (UTAD): implications for prevention and curative therapy. J Mol Psychiatry 2016, https://jmolecularpsychiatry.biomedcentral.com/articles/10.1186/s40303-016-0018-8
ii Ishii N et al: Low risk of male suicide and lithium in drinking water. J Clin Psychiatry 2015: 76:319-326, https://pubmed.ncbi.nlm.nih.gov/25700119/; Zarse K et al: Low-dose lithium uptake promotes longevity in humans and metazoans. Eur J Nutr 2011: 50:387-389, https://pubmed.ncbi.nlm.nih.gov/21301855/; Terao T: Is lithium potentially a trace element? World J Psychiatry 2015: 5:1-3, https://www.wjgnet.com/2220-3206/full/v5/i1/1.htm
iii https://iris.who.int/bitstream/handle/10665/341728/9789240026643-eng.pdf; https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/20220930.htm
iv Gómez-Bernal G: Lithium for the 2019 novel coronavirus. Medical Hypotheses 2020, https://doi.org/10.1016/j.mehy.2020.109822; Qaswal AB et al: The Potential Role of Lithium as an Antiviral Agent against SARS-CoV-2 via Membrane Depolarization: Review and Hypothesis. Sci Pharm 2021, https://doi.org/10.3390/scipharm89010011; Murru A et al: Lithium's antiviral effects: a potential drug for CoViD-19 disease? Int J Bipolar Disord 2020, www.ncbi.nlm.nih.gov/pmc/articles/PMC7239605; Snitow ME et al: Lithium and Therapeutic Targeting of GSK-3. Cells 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC7910927
v Harrison SM et al: Lithium chloride inhibits the coronavirus infectious bronchitis virus in cell culture. Avian Pathol 2007, 36:109-114, https://www.tandfonline.com/doi/full/10.1080/03079450601156083
vi Murru A et al: Lithium's antiviral effects: a potential drug for CoViD-19 disease? Int J Bipolar Disord 2020, https://pubmed.ncbi.nlm.nih.gov/32435920/; Gómez-Bernal G: Lithium for the 2019 novel coronavirus. Medical Hypotheses 2020, https://doi.org/10.1016/j.mehy.2020.109822
vii Spuch C et al: Does Lithium Deserve a Place in the Treatment Against COVID-19? A Preliminary Observational Study in Six Patients, Case Report. Front Pharmacol 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7481472/
viii Spuch C et al: Efficacy and Safety of Lithium Treatment in SARS-CoV-2 Infected Patients. Front Pharmacol 2022, https://www.frontiersin.org/articles/10.3389/fphar.2022.850583/full
ix Freland L & Beaulieu JM: Inhibition of GSK3 by lithium, from single molecules to signaling networks. Front Mol Neurosci 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3282483; Sarkar S et al: Lithium induces autophagy by inhibiting inositol monophosphatase. J Cell Biol 2005, 170:1101-1111, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2171537/; Brown KM & Tracy DK: Lithium: the pharmacodynamic actions of the amazing ion. Ther Adv Psychopharmacol 2013, 3:163-176, https://pubmed.ncbi.nlm.nih.gov/24167688/
x Snitow ME et al: Lithium and Therapeutic Targeting of GSK-3. Cells 2021, https://www.mdpi.com/2073-4409/10/2/255
xi Parry PI et al: 'Spikeopathy': COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. Biomedicines 2023, https://www.mdpi.com/2227-9059/11/8/2287
xii Rong Z et al: SARS-CoV-2 Spike Protein Accumulation in the Skull-Meninges-Brain Axis: Potential Implications for Long-Term Neurological Complications in post-COVID-19. bioRxiv 2023, https://www.biorxiv.org/content/10.1101/2023.04.04.535604v1
xiii Zhao Y et al: SARS-CoV-2 spike protein interacts with and activates TLR4. Cell Res 2021, 31:818-820, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7975240/; Shirato K, Kizaki T. SARS-CoV-2 spike protein S1 subunit induces pro-inflammatory responses via toll-like receptor 4 signaling in murine and human macrophages. Heliyon 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7887388/
xiv Liu ZM et al: Toll-like receptor (TLRs) agonists and antagonists for COVID-19 treatments. Front Pharmacol 2022, https://www.frontiersin.org/articles/10.3389/fphar.2022.989664/full
xv Snitow ME et al: Lithium and Therapeutic Targeting of GSK-3. Cells 2021, https://www.mdpi.com/2073-4409/10/2/255
xvi Nehls M: Unified theory of Alzheimer's disease (UTAD): implications for prevention and curative therapy. J Mol Psychiatry 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4947325/
xvii Duda P et al: GSK3β: A Master Player in Depressive Disorder Pathogenesis and Treatment Responsiveness. Cells 2020, doi: 10.3390/cells9030727.
xviii Fontes-Dantas FL et al: SARS-CoV-2 Spike protein induces TLR4-mediated long-term cognitive dysfunction recapitulating post-COVID-19 syndrome in mice. Cell Rep 2023, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9935273/
xix Nehls M: Unified theory of Alzheimer's disease (UTAD): implications for prevention and curative therapy. J Mol Psychiatry 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4947325/
xx Vavougios GD et al: Type I interferon signaling in SARS-CoV-2 associated neurocognitive disorder (SAND): Mapping host-virus interactions to an etiopathogenesis. Front Neurol 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9771386/; Frank MG et al: SARS-CoV-2 spike S1 subunit induces neuroinflammatory, microglial and behavioral sickness responses: Evidence of PAMP-like properties. Brain Behav Immun 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8667429/
xxi Fleshner M et al: Danger Signals and Inflammasomes: Stress-Evoked Sterile Inflammation in Mood Disorders. Neuropsychopharmacology. 2017, 42:36-45, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5143484/
xxii Wang S et al: Associations of Depression, Anxiety, Worry, Perceived Stress, and Loneliness Prior to Infection With Risk of Post-COVID-19 Conditions. JAMA Psychiatry 2022, 79:1081-1091, https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2796097
xxiii Gould TD et al: In vivo evidence in the brain for lithium inhibition of glycogen synthase kinase-3. Neuropsychopharmacology. 2004, 29:32-38, https://pubmed.ncbi.nlm.nih.gov/12942141/; Jope RS. Lithium and GSK-3: one inhibitor, two inhibitory actions, multiple outcomes. Trends Pharmacol Sci 2003, 24:441-443, https://pubmed.ncbi.nlm.nih.gov/12967765/; Ryves WJ & Harwood AJ: Lithium inhibits glycogen synthase kinase-3 by competition for magnesium. Biochem Biophys Res Commun 2001, 280:720-725, https://pubmed.ncbi.nlm.nih.gov/11162580/
xxiv https://clinicaltrials.gov/study/NCT05618587
xxv https://www.buffalo.edu/news/releases/2023/01/002.html
xxvi Motoi Y et al: Lithium and autophagy. ACS Chem Neurosci 2014, 5:434-442, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4063500/
xxvii Vidoni C et al: Targeting autophagy with natural products to prevent SARS-CoV-2 infection. J Tradit Complement Med 2022, 12:55-68, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8516241/
xxviii Halma MTJ et al: Strategies for the Management of Spike Protein-Related Pathology. Microorganisms 2023, https://doi.org/10.3390/microorganisms11051308; Halma MTJ et al: Exploring Therapeutic Applications of Autophagy in Spike Protein-Related Pathology. 2023, https://www.preprints.org/manuscript/202306.1306/v1
xxix Yang K et al: The Key Roles of GSK-3β in Regulating Mitochondrial Activity. Cell Physiol Biochem 2017, 44:1445-1459, https://karger.com/cpb/article-pdf/44/4/1445/2446568/000485580.pdf
xxx Hamstra SI et al: Beyond its Psychiatric Use: The Benefits of Low-dose Lithium Supplementation. Curr Neuropharmacol 2023, 21:891-910, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10227915/
xxxi Tam ZY et al: Effects of lithium on age-related decline in mitochondrial turnover and function in Caenorhabditis elegans. J Gerontol A Biol Sci Med Sci 2014, 69:810-820,
xxxii Young W: Review of lithium effects on brain and blood. Cell Transplant 2009, 18:951-975, https://journals.sagepub.com/doi/10.3727/096368909X471251
xxxiii Palmos AB et al: Lithium treatment and human hippocampal neurogenesis. Transl Psychiatry 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8557207/
xxxiv Nunes MA et al: Microdose lithium treatment stabilized cognitive impairment in patients with Alzheimer's disease. Curr Alzheimer Res 2013, 10:104-107, https://www.researchgate.net/publication/228098677
xxxv Enderle J et al: Plasma Lithium Levels in a General Population: A Cross-Sectional Analysis of Metabolic and Dietary Correlates. Nutrients 2020, https://www.mdpi.com/2072-6643/12/8/2489
xxxvi https://www.imd-berlin.de/fachinformationen/diagnostikinformationen/lithium-ein-essentielles-spurenelement (zuletzt abgerufen am 2.11.2023)
xxxvii Seidel U et al: Lithium-Rich Mineral Water is a Highly Bioavailable Lithium Source for Human Consumption. Mol Nutr Food Res 2019, https://pubmed.ncbi.nlm.nih.gov/31051049/
xxxviii Chassard-Bouchaud C et al: Bioaccumulation de lithium par les organismes marins des zones côtières européennes, américaines et asiatiques: étude microanalytique par émission ionique secondaire [Bioaccumulation of lithium by marine organisms in European, American, and Asian coastal zones: microanalytic study using secondary ion emission]. C R Acad Sci III 1984;299:719-724, https://pubmed.ncbi.nlm.nih.gov/6440674/; Barbosa H et al: Lithium: A review on concentrations and impacts in marine and coastal systems. Sci Total Environ 2023, https://www.sciencedirect.com/science/article/pii/S0048969722064737
xxxix Marshall TM: Lithium as a nutrient. J Am Phys Surg 2015, 20: 104–109, https://www.jpands.org/vol20no4/marshall.pdf; Szklarska D & Rzymski P: Is Lithium a Micronutrient? From Biological Activity and Epidemiological Observation to Food Fortification. Biol Trace Elem Res 2019, 189:18-27, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6443601/
xl https://www.researchgate.net/profile/Gerald-Rimbach/publication/341287028_Lithium_Li_concentrations_gL_in_381_German_mineral_and_medicinal_waters/data/5eb923af92851cd50da8b66e/Suppl-AllMIneralwaterRG.pdf?origin=publication_list
xli Seidel U et al: Lithium-Rich Mineral Water is a Highly Bioavailable Lithium Source for Human Consumption. Mol Nutr Food Res 2019, https://onlinelibrary.wiley.com/doi/10.1002/mnfr.201900039
xlii https://www.foodwatch.org/fileadmin/foodwatch.de/news/Uran-in-Mineralwasser_20090518_01.pdf; http://www.osmose-wasser.com/Uranbelastung.html
xliii Rüthrich HL et al: Memory retention in old rats: improvement by orotic acid. Psychopharmacology (Berl) 1983, 79:348-351, https://pubmed.ncbi.nlm.nih.gov/6407051/
xliv Pacholko AG & Bekar LK: Lithium orotate: A superior option for lithium therapy? Brain Behav 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8413749/
xlv Pacholko AG & Bekar LK: Different pharmacokinetics of lithium orotate inform why it is more potent, effective, and less toxic than lithium carbonate in a mouse model of mania. J Psychiatr Res 2023, 164:192-201, https://www.sciencedirect.com/science/article/pii/S0022395623003102
xlvi Murbach TS et al: A toxicological evaluation of lithium orotate. Regul Toxicol Pharmacol 2021, https://www.sciencedirect.com/science/article/pii/S0273230021001136
xlvii Young W: Review of lithium effects on brain and blood. Cell Transplant 2009, 18:951-975, https://journals.sagepub.com/doi/10.3727/096368909X471251
xlviii Spuch C et al: Efficacy and Safety of Lithium Treatment in SARS-CoV-2 Infected Patients. Front Pharmacol 2022, https://www.frontiersin.org/articles/10.3389/fphar.2022.850583/full
xlix Pacholko AG & Bekar LK: Different pharmacokinetics of lithium orotate inform why it is more potent, effective, and less toxic than lithium carbonate in a mouse model of mania. J Psychiatr Res 2023, 164:192-201, https://pubmed.ncbi.nlm.nih.gov/37356352/
l Pacholko AG & Bekar LK: Lithium orotate: A superior option for lithium therapy? Brain Behav 2021, https://onlinelibrary.wiley.com/doi/10.1002/brb3.2262
li https://www.klinik-st-georg.de/lithium-ein-wichtiges-mineral-mit-breiter-klinischer-wirkung/ (zuletzt abgerufen am 3.11.2023)
Interesting article, thanks. Lithium and Lithium Orate is sold w/o prescription. One company is https://www.lifeextension.com.
Can anyone here clarify for me how much lithium orotate to take to obtain the recommended 1 mg of pure lithium? My confusion stems from the fact that every lithium supplement I can find in the U.S. is either 1 mg or 5 mg. of lithium orotate. The capsules I have say they are 1000 mcg (1 mg.) of lithium as lithium orotate. Does this mean the capsule actually contains 23 mg of lithium orotate, which is equivalent to 1 mg. of pure lithium? So I would take one of these daily to obtain the 1 mg of pure lithium for prevention of lithium-deficiency-related diseases? I don't know how to tell whether this capsule contains 1 mg. of pure lithium or 1 mg. of lithium orotate, which would require 23 capsules to get 1 mg of pure lithium.